



As states continue to introduce laws that restrict access to gender-affirming care or limit protections against conversion therapy, questions have arisen about the effectiveness of interventions intended to help transgender youth. In this political climate, gold-standard evidence is more important than ever.
Prior research has been unable to tease out cause and effect between health outcomes and gender-affirming care like hormone therapy or gender-denying interventions like conversion therapy, largely because of a lack of longitudinal data or an appropriate control group. To establish whether something causes an outcome, researchers typically rely on randomized control trials – experiments that randomly assign people to a treatment or a placebo. Random assignment is a trusted way to create two equal groups to compare. However, because it is unethical to withhold treatment or administer potential harmful interventions, randomized controls trials are off the table in this case.
In lieu of randomized control trials, researchers often retrospectively compare people who have received an intervention with those who did not. Studies using this approach have linked hormone therapy with positive mental health outcomes for trans teens. However, because this treatment requires parental approval, teens who receive hormone therapy may have more supportive families than those who do not. The mental health improvement they experienced may partially be due to living in a gender-affirming family environment rather than the effects of hormone therapy alone.
Our research team was able to address these study design issues directly. Along with our colleagues Duc Hien Nguyen and Yana Rodgers, we are economics and health policy researchers who study the health and economic outcomes of marginalized populations, including LGBTQ+ communities. To assess cause and effect, we used a method commonly used in economics, policy analysis and health policy research called an event study. We analyzed data from the 2015 U.S. Transgender Survey, which includes responses from over 27,000 trans adults across the nation. We compare people who initiate an intervention with those who initiate the same intervention one year later. The group that has not yet started treatment acts as a control group, providing credible estimates of the effect of treatment.
We found that supportive family environments and hormone replacement therapy that affirms a transgender child’s gender identity decrease their risk of suicide or running away from home, whereas unsupportive family environments and conversion therapy that denies their gender identity increase these risks.
Many transgender people experience gender dysphoria, which is psychological distress arising from a mismatch between how a person expresses their gender identity and the social norms of their sex assigned at birth. To treat gender dysphoria, health professionals typically use gender-affirming interventions such as hormone therapy to align gender expression with identity. Some, however, use gender-denying interventions such as conversion therapy to align gender identity with sex.
Gender affirmation includes processes that help a person feel socially and physically aligned with their gender identity. Affirmation could include social changes, such as going by a gender-affirming name and pronouns, using gender-aligned bathrooms, or wearing gender-affirming clothing. Affirmation could also include medical interventions, such as medications to delay the onset of puberty, hormones that help align physical characteristics with gender identity, or, for trans adults, gender-affirming surgeries. Some trans adults also legally change their names and gender markers on their ID. Research has shown that these forms of gender affirmation may alleviate gender dysphoria.
Conversely, gender-denying interventions like conversion therapy attempt to change the sexual orientation or gender identity of youth. These interventions assume that gender identity is malleable before puberty. Although it is presumably intended to alleviate gender dysphoria and social stigma of being trans, studies have found that it can prolong and intensify those issues and lead to psychological distress in adulthood.
Because there is no credible evidence supporting the efficacy of conversion therapy, many professional health organizations have recommended gender-affirming care to alleviate gender dysphoria in trans people.
There has been limited evidence, however, on the health effects of both hormone therapy and conversion therapy for trans people, which is why the Centers for Medicare and Medicaid Services has not provided a national coverage determination regarding hormone replacement therapy. This means HRT isn’t uniformly covered by state or federal health insurance.
So what are the effects of affirming or denying a child’s gender identity?
First, we found that over 40% of trans adolescents living in family environments that are unsupportive of their gender identity attempted suicide by the age of 18, a rate approximately eight times as high as that of cisgender adolescents.


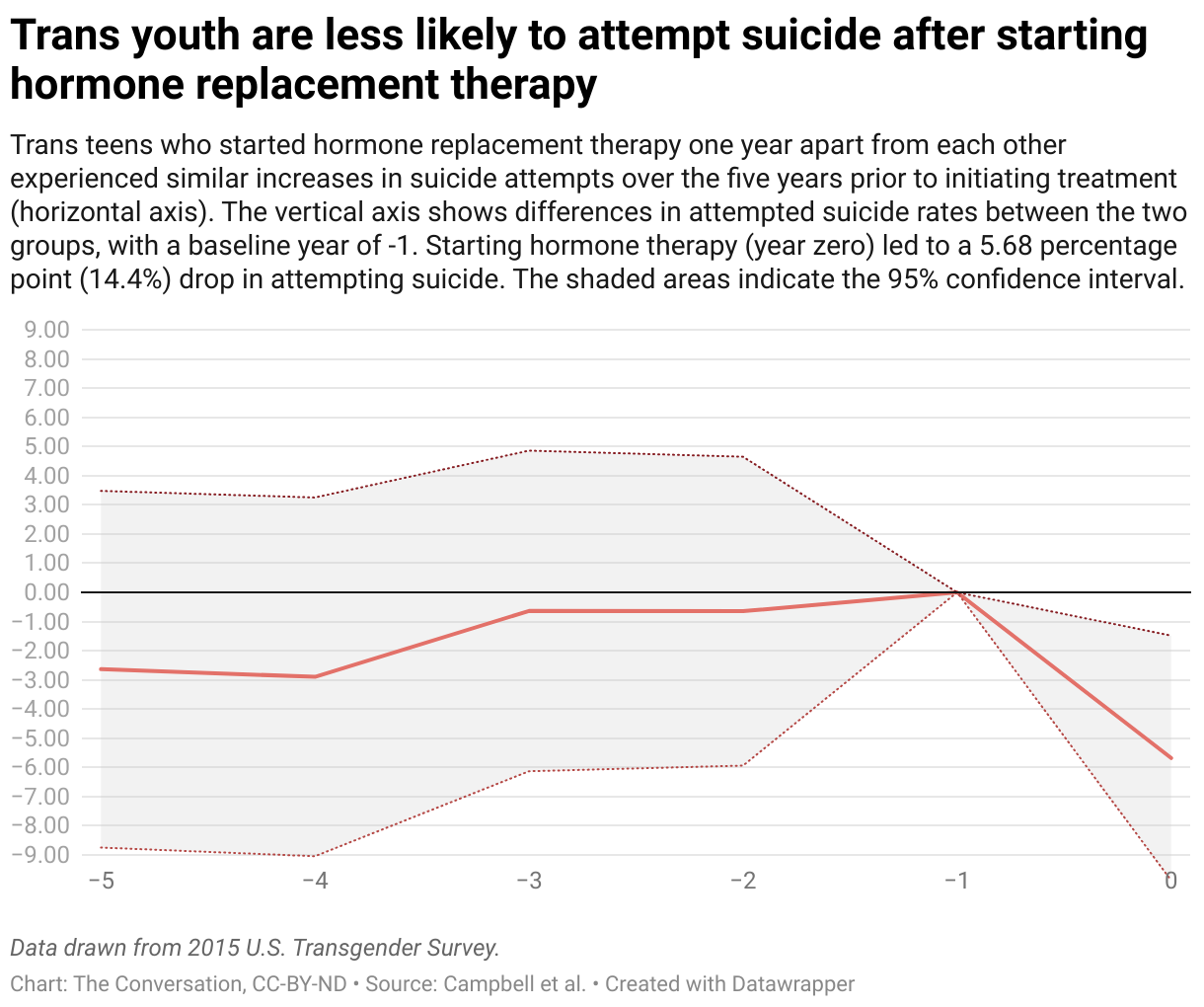
We also found that hormone replacement therapy significantly improves the mental health of trans youths. In comparing differences in suicide attempts between trans youths who started HRT a year apart from each other, we found that both groups experienced similar increases in suicide attempts over the five years before initiating treatment but experience a significant drop the year they start treatment. Overall, initiating hormone therapy led to a 14.4% reduction in attempting suicide for trans youths.
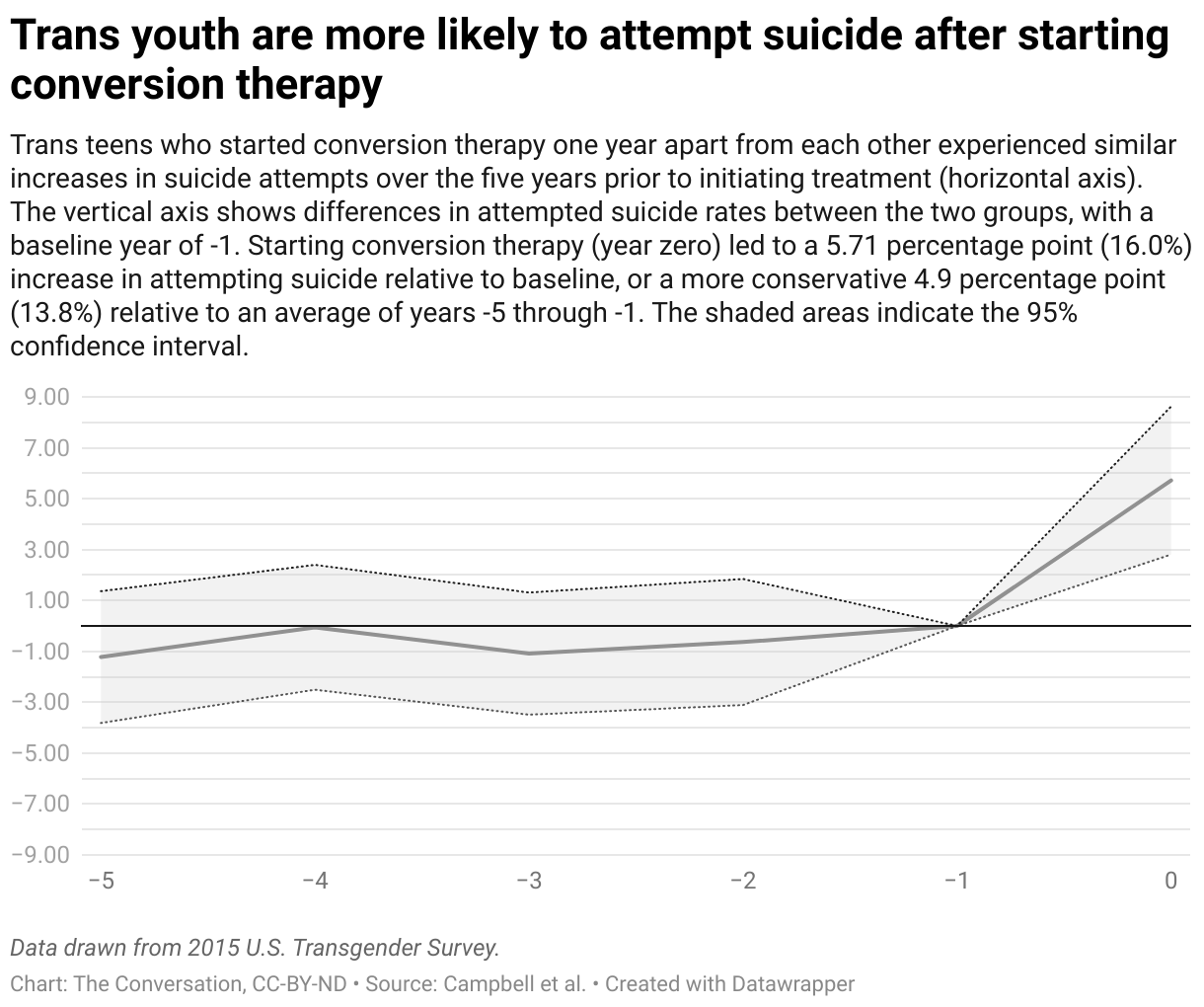
Our research on the effects of conversion therapy on the mental health of transgender youths had dismal findings. We found a 13.8% increase in attempted suicide within the first year of conversation therapy, and a 47.5% increase in running away from home.
We also analyzed the effects of social transitions on risk of attempting suicide or running away from home. These social transitions include realizing their gender differed from their sex assigned at birth, self-identification as trans, starting to tell others they are trans, and living full time as their gender identity.
We found that for trans youths living with unsupportive families, social transitions increase their risk of attempting suicide and running away from home. For those living in supportive family environments, that risk is reduced and in some cases virtually eliminated. Some of the increased risk of suicide and running away from home for trans youths living in unsupportive family environments can likely be attributed to higher incidences of conversion therapy and limited access to hormone therapy.
Transgender people face widespread stigma, discrimination and violence. In June 2023, the Human Rights Campaign declared a national state of emergency for LGBTQ+ Americans, the first in the LGBTQ civil rights organization’s over 40-year history. This was prompted by the more than 560 anti-transgender bills that have been introduced in the U.S. through July 2023, 80 of which have passed.
More anti-trans bills have been on the docket in 2023 than any prior year in U.S. history. Our research suggests that policies restricting access to gender-affirming care and limiting protections against conversion therapy will have significant negative effects on the lives of transgender youths.
As newer and larger data sets on the health, economic and social outcomes of trans people become available, researchers will be able to quantify the effects of anti-trans policies and provide richer insights into the lives of transgender Americans. Whether these findings will help change the tide of restrictive policies on trans health care and protections in the U.S. remains to be seen, but for now, our research suggests that family support will be key.
If you are struggling or having suicidal thoughts, help is available. Call or text the 988 Suicide & Crisis Lifeline or chat at 988lifeline.org. The Trans Lifeline (1-877-565-8860) and The Trevor Project (phone 1-866-488-7386, text 678-678, or chat thetrevorproject.org also offer crisis support.
This article is republished from The Conversation, an independent nonprofit news site dedicated to sharing ideas from academic experts. If you found it interesting, you could subscribe to our weekly newsletter.
Read more: Gender-affirming care has a long history in the US – and not just for transgender people I’m a pediatrician who cares for transgender kids – here’s what you need to know about social support, puberty blockers and other medical options that improve lives of transgender youth
Nathaniel Tran receives funding from the National Institute on Aging.
Samuel Mann receives funding from the Nuffield Foundation.
Travis Campbell does not work for, consult, own shares in or receive funding from any company or organization that would benefit from this article, and has disclosed no relevant affiliations beyond their academic appointment.
![]()
